What works to improve mental wellbeing in the UK: insights from WEMWBS
Downloads
In partnership with

Introduction
As a What Works Centre we bring together high quality wellbeing evidence to support decision-making and the delivery of more effective and efficient services. We use the UK’s harmonised wellbeing standards to inform our evidence reviews and understand what can be done to improve wellbeing and reduce its inequalities. The national measures within the harmonised standards include subjective wellbeing, mental wellbeing and social capital measures, all of which are commonly used in national and local outcomes frameworks. They help us build a shared knowledge base that uses consistent and comparable wellbeing constructs.
Our Rapid Reviews:
- Explore what is known so far about what works, for whom and in what contexts.
- Illustrate how wellbeing measures are used in different studies so we can support organisations to generate high quality findings.
- Conduct rigorous searches using less extensive methods when compared to systematic reviews, but often searching across grey and published sources.
In 2020, we reviewed evaluations using the ONS4 Personal Wellbeing measures. For this current project, the Centre worked with Kohlrabi Consulting to conduct a 6-month rapid review of UK interventions, delivered from 2007 to the present, that aim to improve mental wellbeing.
The big picture: WEMWBS scales as a key starting point for mental wellbeing
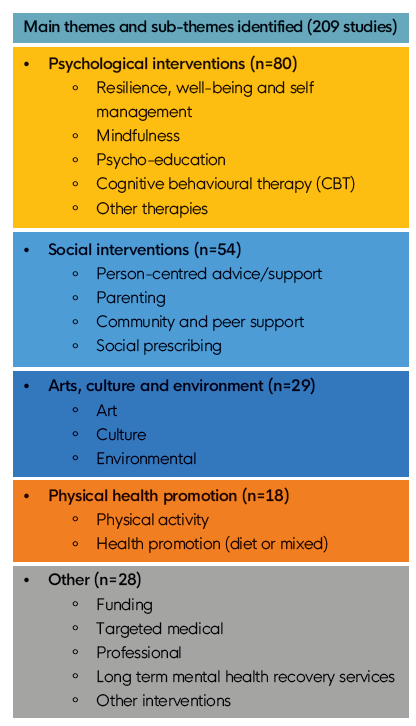
Findings on what works to improve mental wellbeing

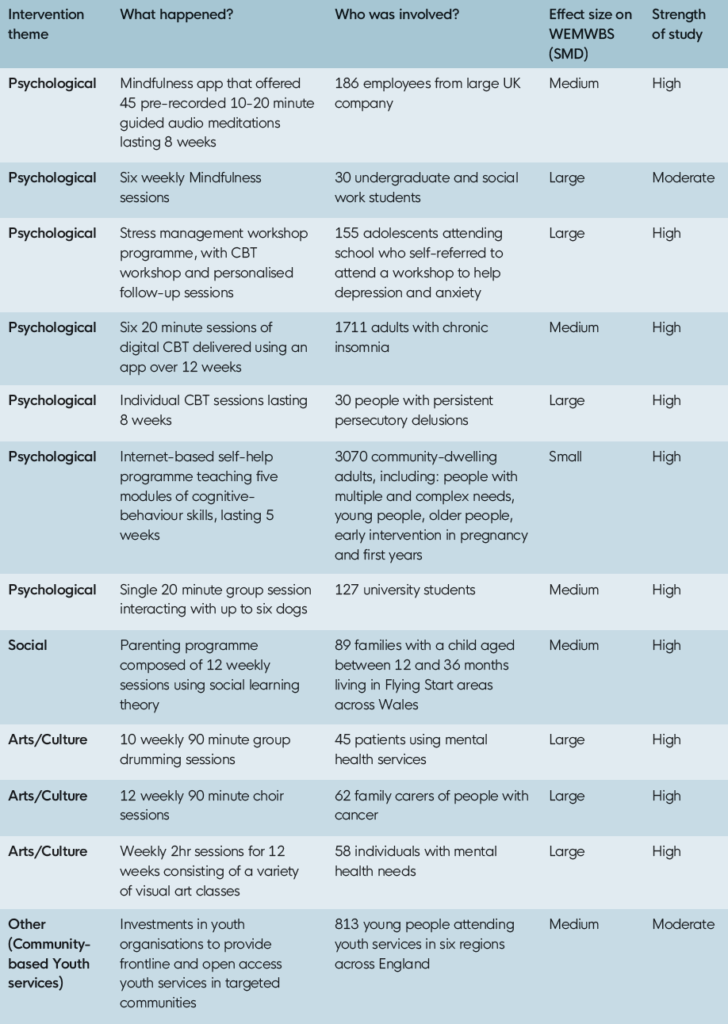
High quality evidence from controlled studies
Approach to meta-analysis
Where and how are the WEMWBS scales used
How robust were the findings?
Implications and recommendations
Policy, practice and commission
Suggested citation
Explore more
![]()
[gravityform id=1 title=true description=true ajax=true tabindex=49]