You may also wish to Read the blog article on this document.
June 2022
What matters for mental health and productivity in a financial services firm?
Downloads

In partnership with

Case study evidence: the quick read
In the organisation studied:
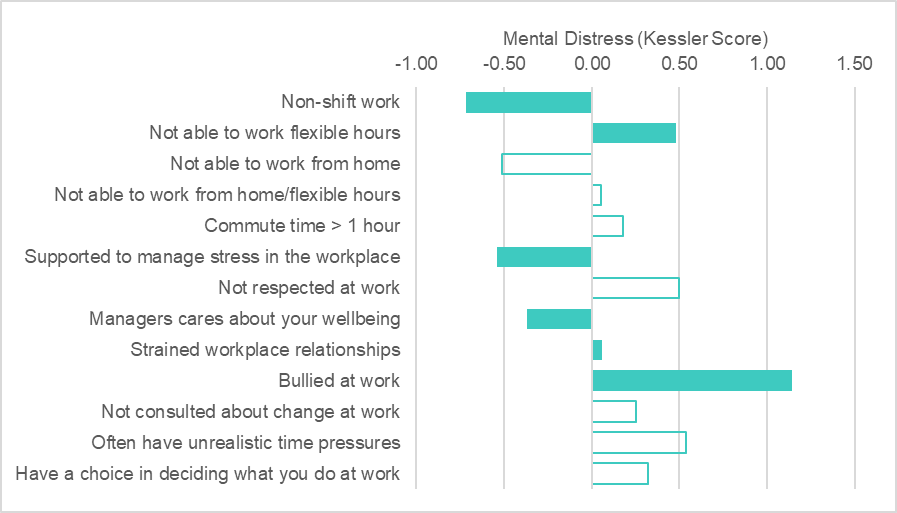
- Poor employee mental health can be related to some job-specific and working-culture characteristics such as: shift work, lack of flexible hours, unsupportive managers and strained working relationships.
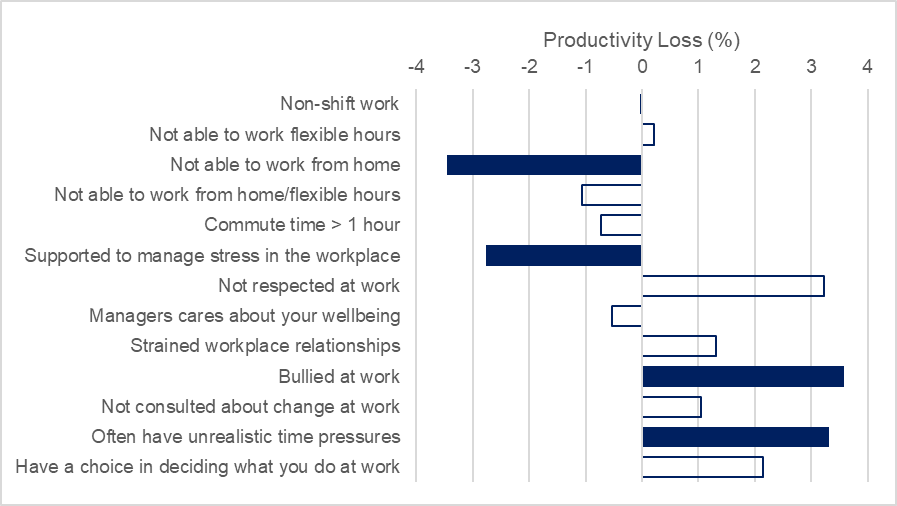
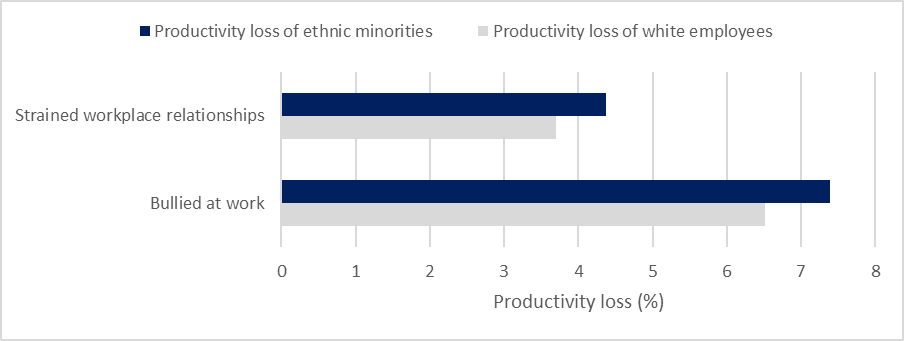
- Bullying and not being supported to manage stress were two factors jointly related to staff mental health and productivity.
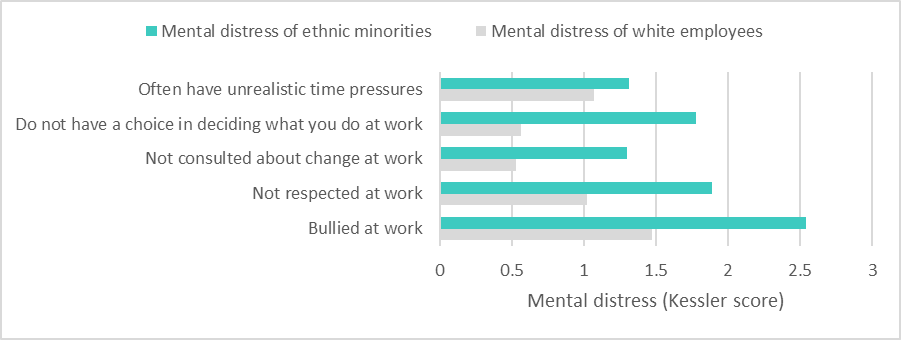
- The negative relationship between poor job quality and mental health and productivity may be stronger for ethnic minorities.
- Working from home increased productivity loss, while unrealistic time pressures were related to decreased productivity loss.
- Findings suggest that roles which have less flexibility need more attention paid to protective factors.
Context
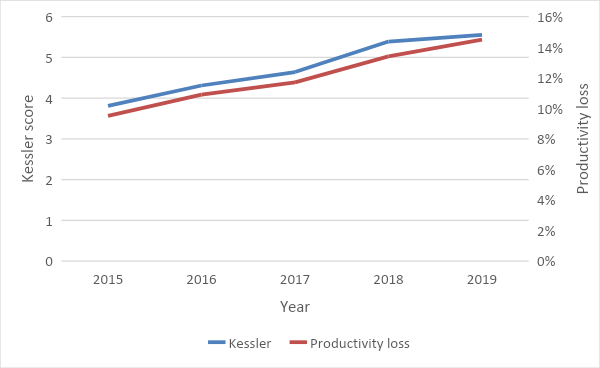
Measurement and outcomes
The study
What we found
Recommendations for action
What we need to know more about
Data and methods: regression analysis with survey data
Suggested citation
![]()
[gravityform id=1 title=true description=true ajax=true tabindex=49]